TABLE OF CONTENT
Custom AI healthcare solutions replace generic, off-the-shelf software with tools built around a specific clinical workflow, such as wound imaging analysis or prior authorization automation. Neuramonks USA builds these systems through a scoped pilot engagement so hospitals and clinics can validate results before committing to a full production build.
Every healthcare administrator evaluating AI right now is facing pressure from three directions at once: fewer staff to do the work, a rising documentation load, and boards asking for a cost-reduction plan with numbers attached. The American Hospital Association's 2026 Workforce Scan names administrative burden and staffing gaps as the top pressures facing hospital leaders this year, and industry reporting citing McKinsey research puts a global figure on what closing the healthcare worker shortage could mean for the economy: roughly $1.1 trillion in added value. That is the backdrop against which most buyers search for AI solutions, usually landing on generic chatbots repackaged for healthcare rather than tools engineered for an actual clinical workflow.
The pattern repeats across specialties. A wound care clinic needs consistent measurement, not a chatbot. A billing office needs prior authorization drafted against payer-specific rules, not a summarizer. A front desk needs intake triage that understands its own scheduling logic, not a generic FAQ bot. Buyers who evaluate AI vendors on demo polish alone tend to discover the gap only after signing, when the tool cannot actually plug into the EHR or imaging system already running the department.
Why Generic AI Tools fail Healthcare Providers
A general-purpose AI assistant can summarize a note or draft an email. It cannot reliably measure a wound from a clinical photo, flag a prior authorization likely to be denied, or route an intake form to the right specialist based on your clinic's specific triage rules. Those are narrow, high-stakes tasks that require a model trained and validated against your data, your documentation standards, and your compliance requirements, not a general model doing its best guess.
This is the gap a custom healthcare AI build is designed to close. Instead of asking staff to adapt their workflow around a generic product, a custom build maps to the EHR, the imaging system, and the documentation format your team already uses. The result is a tool clinicians actually open, not one more login they avoid. It also means fewer support tickets down the line, because the system was validated against your own edge cases before launch rather than a generic sample dataset.
There is a second, quieter cost to generic tools: liability. A wound measurement that is off by even a few millimeters, repeated across hundreds of patient visits, can distort a wound-healing trend line that a physician relies on to decide whether a treatment plan is working. A prior authorization draft that misreads payer rules can delay care by weeks. Generic tools are built to be broadly useful. Clinical workflows need to be precisely correct for the one use case they serve.
Stop Planning AI.
Start Profiting From It.
Every day without intelligent automation costs you revenue, market share, and momentum. Get a custom AI roadmap with clear value projections and measurable returns for your business.
What a Custom-Built Healthcare AI System Actually Solves
Medical Imaging and Wound Care Analysis
Wound care is a clear example of where generic tools fall short. Manual wound measurement is slow, inconsistent between clinicians, and hard to track over time across multiple visits. Neuramonks built an automated wound detection and measurement system using deep learning that analyzes clinical photos to detect wound boundaries and calculate measurements automatically, giving clinicians a consistent, repeatable reading instead of a manual tape-measure estimate that varies by who is holding it.
Clinical Documentation and Prior Authorization
Documentation and prior authorization consume hours of clinician and staff time every week. A custom AI healthcare solution can draft visit notes from a conversation, flag missing information a payer is likely to reject, and pre-fill authorization requests against payer-specific rules, cutting the manual review time down to a final check rather than a full rebuild.
Patient Intake and Triage
Front-desk and call-center staff spend significant time on repetitive intake questions before a patient ever reaches a clinician. An AI agent handling structured intake, appointment routing, and basic triage questions frees that staff time for tasks that actually need a human, particularly during the seasonal volume spikes that strain most practices.
Data handling is built around HIPAA, not bolted on after
A qualified AI development partner designs access controls, data residency, and audit logging into the system architecture from the first technical decision. Retrofitting compliance after a generic product is already built is where most healthcare AI projects run into trouble during a security review.
AI Proof of Concept Services: proof before you commit
Few healthcare leaders want to sign a six-figure contract for a system nobody has tested against their own data. That is the reasoning behind scoping a smaller pilot first: pick one workflow, such as wound measurement or intake triage, run it against real (de-identified) patient data for four to eight weeks, and measure the result before expanding the build. If the pilot does not perform, you have lost a fraction of what a full commitment would have cost. If it does, you now have evidence, not a vendor's promise, to bring to your board.
How to evaluate a healthcare AI development partner
Bring these questions into the first vendor call, before any contract discussion:
- Can you show a clinical or operational system you built that is running in production today, not just a pilot?
- How do you handle HIPAA and data residency in the system architecture, specifically?
- What does a scoped pilot look like for our specific workflow, and what would we measure to decide whether to scale it?
- Who owns the model outputs and the underlying data once the engagement ends?
- What does support look like six months after launch, once the initial contract is over?
A vendor who answers with named examples and specific numbers is signaling real experience. A vendor who answers with reassurance and marketing language is signaling the opposite, regardless of how polished the demo looked.
Early Research Versus an Active Buying Decision
Not every reader of a guide like this is choosing between finalists this month. Some administrators are early in the process: gathering internal support, building a business case, or figuring out which workflow to test first before procurement gets involved. Others already know they want a wound-care imaging tool or a documentation assistant and are comparing two or three vendors directly.
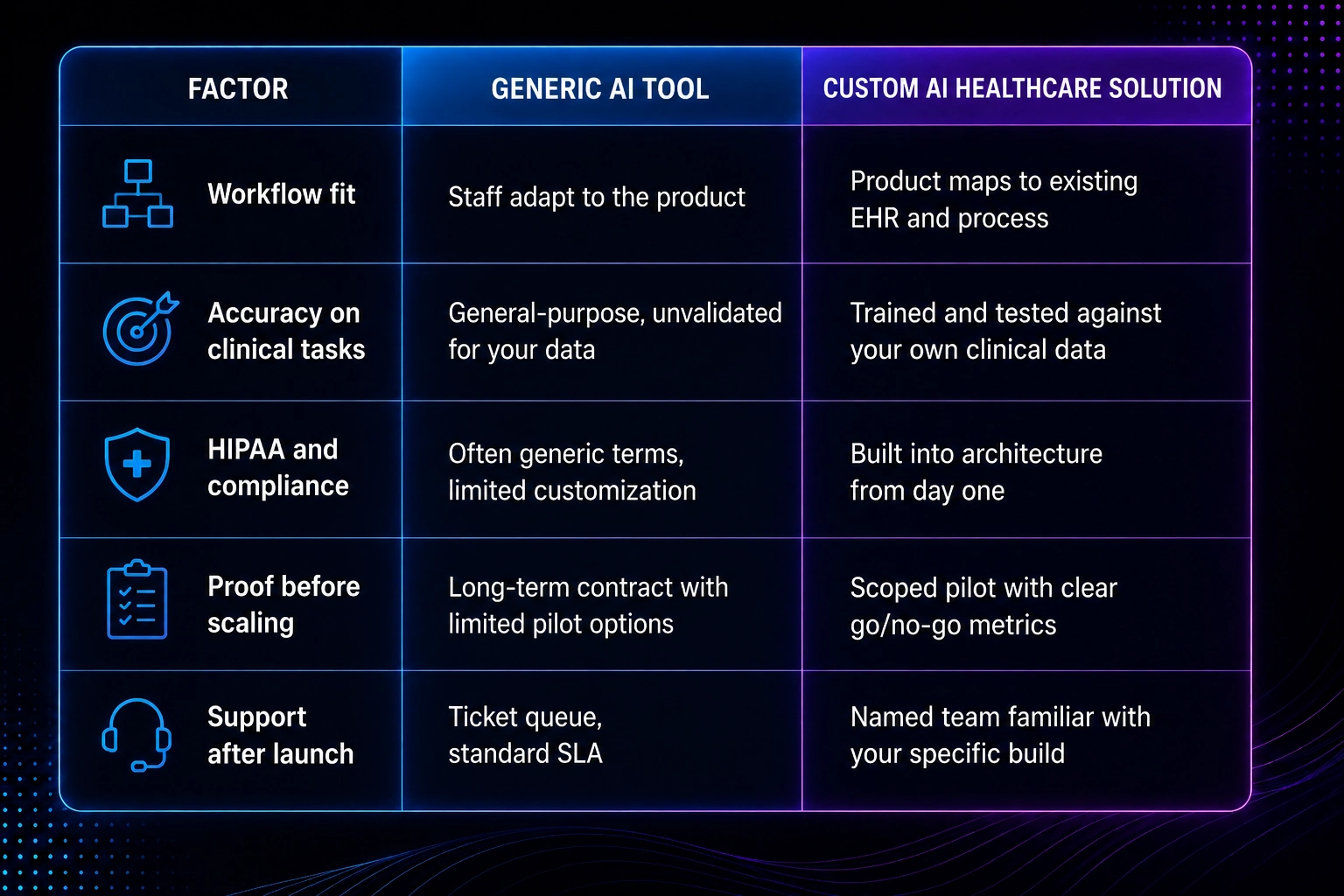
Both groups can use the same framework. If you are early, use the comparison table above to build an internal scorecard so stakeholders are judging vendors against agreed criteria instead of demo polish. If you are closer to a decision, take the five questions above into your finalist calls and ask each vendor to answer in writing, so you have something concrete to compare once the calls are over.
What the Results Actually Look like
Numbers matter more than a demo. we documented how a healthcare operations team applied automation to reduce administrative overhead in How Healthcare Agencies Cut Operational Costs by 40%, and What It Actually Takes to Get There, which breaks down the specific workflow changes behind that figure rather than presenting the percentage on its own. Read it alongside the wound detection case study above if you want to see both a clinical and an operational example before scoping your own pilot.
Custom Build Versus Generic Tool, side by side
Why Neuramonks is Built for this Work
Neuramonks USA builds AI healthcare solutions for hospitals, clinics, and diagnostic centers, with delivery teams across the US, India, and the UAE working on Agentic AI, RAG development, Computer Vision, and AI Automation projects specifically scoped to healthcare, manufacturing, and construction clients. The wound detection system referenced above is one example of that clinical, deep-learning work already running in production, not a hypothetical capability described in a sales deck.
Engagements open with a discovery call focused on one workflow, not a full department rebuild. That keeps the first conversation short and the first commitment small, which matters when the person evaluating vendors also has to justify the spend to a CFO or a board that has seen AI promises fall short before.
If you are scoping a pilot for your organization, book a free consultation with the Neuramonks USA team and bring the specific workflow you want tested first.